Nanomedicine, Volume IIA: Biocompatibility
© 2003 Robert A. Freitas Jr. All Rights Reserved.
Robert A. Freitas Jr., Nanomedicine, Volume IIA: Biocompatibility, Landes Bioscience, Georgetown, TX, 2003
15.5.1.2 Epidermalgia and Allodynia
Will epidermal penetration by nanorobots produce a sensation of pain (epidermalgia) in the human patient? Modern hypodermic needles have outside diameters of >200 microns (33 gauge) [3687] and can barely be felt penetrating the skin. Most of the sensation generated by fine needle stick can probably be attributed to subdermal needle cantilevering motions rather than skin penetration per se. (The smallest solid acupuncture needles are ~120-180 microns in diameter [3688] and there is generally little or no sensation of pain upon insertion of the needle* which sometimes produces analgesia [3689].) Hypodermic injections can also produce a sensation of fluid flowing into the veins, probably due to: (1) a thermal and viscosity mismatch between injecta and venous blood, (2) a slight vein expansion from the local rise in fluid pressure, (3) fluid shear forces (e.g., in dialysis needles [3690]), and (4) in some cases a direct chemical response [3691].
* Acupuncture needles have a doweled end, not a cutting end like most hypodermic needles, thus may be less likely to cause tissue damage, vascular puncture, or bruising when inserted [3692]. The needling sensation (de qi) is thought to be caused by muscle fibers being caught and twisted on the needle tip [3693].
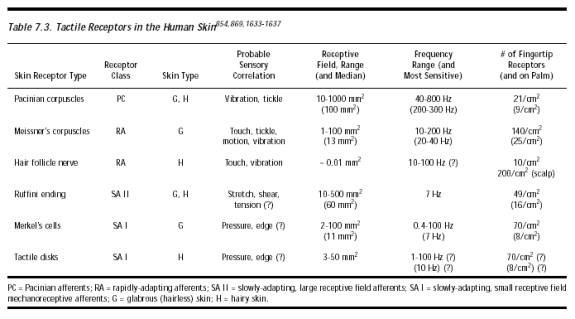
Nanorobots which are 1-10 microns in diameter present far smaller dermal penetration footprints than a hypodermic needle and thus should produce a stimulus even farther below the threshold of sensibility than a needle. They should induce no detectable cantilevering motions because tissue-transiting nanorobot convoys (Section 15.5.2.3) need not be flexurally rigid. As with tickle (Section 9.5.2) and itch (Section 15.5.1.1) sensations, individual nanorobots appear unlikely to exert sufficient forces to elicit sensations of stretch from Ruffini endings [3694]. Equally unlikely are pressure sensations from other mechanoreceptive afferents in the skin [3695] even if the nerve is directly contacted, itself an improbable occurrence given the typical number density of <1 afferents/mm2 in the skin (Table 7.3). Flow sensations also should be minimized because nanorobots may be self-injecting without carrier fluid or without motion of carrier fluid (Chapter 16) thus minimizing vein expansion. Nanorobots can also self-heat to blood temperature during injection, and should be chemically inert. Nanocatheters and nanocannula (Chapter 19) larger than ~100 microns in diameter and major nanosurgical interventions (Chapter 12) may require analgesic auxiliaries to entirely suppress epidermalgia during the procedure.
Allodynia – including nanorobot-induced cutaneous tactile allodynia [3696, 3697], mechanical allodynia [3698], mechanical hyperalgesia [3699] or mechanical hyperesthesia [3700] – might be possible in unusual circumstances when a normally painless stimulus such as hair deflection is perceived as painful. (An extreme example is reflex sympathetic dystrophy [5597] or RSD.) In one experiment [3701], median threshold of A fiber nociceptors to monofilament stimulation was in the range 207-1639 kPa (mean 744 kPa) and 130-764 kPa (mean 411 kPa) for the C fibers, thus requiring allodyniagenic pressures >1 atm. Hair follicle nerves have a receptive field of ~0.01 mm2 (Table 7.3), hence >1 mN nanorobotic forces may need to be applied near the base of the hair shaft to induce allodynia. Under normal circumstances not involving crinal aerobots (Chapter 28), this seems unlikely. The threshold for first sensation during esophageal wall distension is ~2900 N/m2, with chest pain ensuing at a threshold distension pressure of ~6100 N/m2 [3702]. Colorectal mechanical allodynia is induced in rats at 1300-5300 N/m2 [3703].
Last updated on 30 April 2004
{kind=link}