Nanomedicine, Volume IIA: Biocompatibility
© 2003 Robert A. Freitas Jr. All Rights Reserved.
Robert A. Freitas Jr., Nanomedicine, Volume IIA: Biocompatibility, Landes Bioscience, Georgetown, TX, 2003
15.6.1 Somatic Intrusiveness
The issue of somatic intrusiveness arises whenever macroscopic quantities of foreign materials or medical nanorobots must be implanted into the human body. What is the maximum volume of foreign material that the body can safely accommodate?
The 70 kg reference human male has a body volume of 0.06 m3 (with ~90% of U.S. males between 0.05-0.10 m3) [5924] but the most rotund man of record, of otherwise normal stature, had a body volume of ~0.50 m3 (Section 8.2). Hence those portions of the body not enclosed by bone in which skin distension readily permits incorporation of new materials may allow the reference male to add, at most, up to ~0.44 m3 of foreign material, or up to ~633% volumetric expansion. It is not asserted here that such additions are necessarily healthy or wise,* but merely that they appear possible within the limits of natural human tissue elasticity. Genetic or other permanent artificial modifications to tissue elasticity or body architecture could further increase the expansibility of the human dermal envelope. Additionally, the dermal expansion that accompanies large weight gains occurs slowly over time, so an immediate expansion of equal volume due to the presence of nanorobots or nanoorgans would not be tolerated as well.
* Macroscopic biocompatible foreign bodies such as pacemakers and orthopedic pins and plates may reside inside the body indefinitely without ill effect, as long as they do not migrate (Section 15.4.1). This is true even in the gut. One case presentation [166] of foreign bodies in the alimentary tract proudly reported: “We present a case of a patient who ingested 648 metallic objects that formed an intertwining mass within the stomach, requiring operative removal. Of interest was the absence of symptoms and complications after 11 years of continual ingestion. To our knowledge, this is the second heaviest accumulation of metallic foreign objects removed from the stomach of a living patient.” (The absence of symptoms might be explained by psychiatric causes.) Another study [159] involving 8 observed cases found that swallowed foreign bodies could be left in the intestine for years without any noticeable distension (e.g., splanchnomegaly) or pain (splanchnodynia).
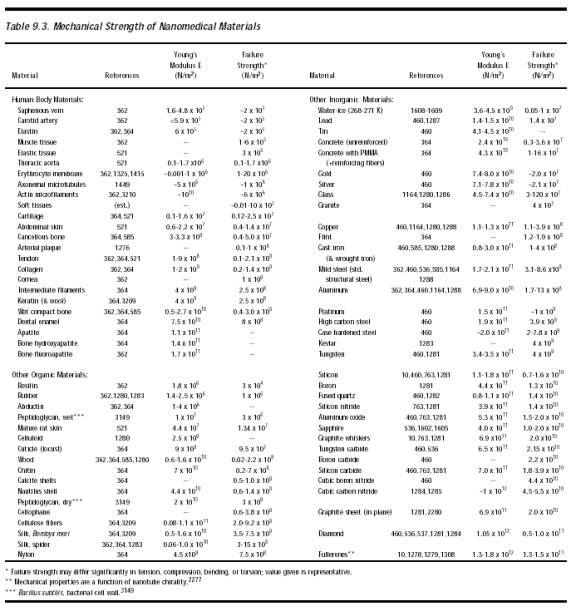
The principal natural limit for skin stretching may be estimated from the elasticity of the thick collagenous connective tissue or dermis – a three-dimensional feltwork of continuous collagen fibers embedded in a protein-polysaccharide matrix in which elastin fibers also are present [4435]. The elastin produces a material with rubber-like elasticity at small extensions but is limited at longer extensions by the dimensions of the collagen framework [4436]. Skin is normally under tension even when not being deformed by motion or other forces. For example, the resting strain in human skin varies from 10-30% [4437], or lambdaskin = 1.1-1.3 where lambdaskin is the ratio of the length of stressed to unstressed skin. Distension is dominated by elastin up to lambdaskin ~ 1.6, but as the tissue is extended further, collagen fibers become aligned in the direction of extension and are stretched by the applied load. By lambdaskin ~ 1.9 at a tensile stress load of ~107 N/m2 (near the failure strength of abdominal skin, or ~0.4-1.4 x 107 N/m2; Table 9.3), the fiber lattice has a high degree of orientation parallel to the direction of extension and the skin becomes mechanically similar to tendon [4435, 4436]. A dermal envelope that encloses a body volume of 0.06 m3 at lambdaskin = 1.2 will enclose ~(1.9/1.2)3 (0.06 m3) ~ 0.24 m3 at lambdaskin = 1.9, an addition of ~0.18 m3 of foreign material or ~300% volumetric expansion. Such extensive and prolonged stretching of the skin (as is common abdominally during pregnancy) can produce dermal itching sensations [4438].
Nanorobots injected into open tissue volumes dominated by extracellular matrix (ECM) also are limited primarily by the elasticity of collagen and elastin fibers that form the scaffolding of the ECM (Section 9.4.4.2). If these matrix fibers can readily stretch by a linear factor of lambdaECM = (lambdastretched / lambdarelaxed) ~ 1.3, where lambdastretched ~ 1.6 [4435, 4436] and lambdarelaxed ~ 1.1-1.3 [4437], then the maximum volumetric expandability of ECM-dominated tissue volumes is ~(lambdaradial3 – 1) = 1.2 (120%). These gross limits are not well explored experimentally. One experiment [1848] in which subdermal rat paw tissue received a 0.3% volumetric implantation of 10- to 20-micron diamond particles provoked only a slight increase in volume of the treated paw relative to the control paw and the edematous effect subsided after 30-60 minutes.
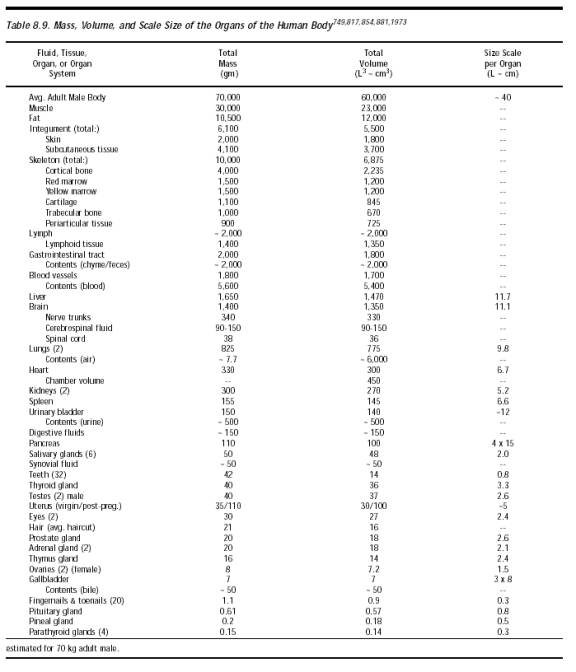
Several organs of the human body regularly expand and contract in volume during their normal functioning. For instance, the two lungs (including the integral tissues) normally cycle between 3.1-3.5 liters in total volume during resting respiration (~13% expansion), but at maximum inspirational capacity the lungs may cycle from 3.1-6.8 liters, a maximum volumetric expansion of ~120%. Similarly, the stomach varies between 0.5 liter when empty to 1.5 liters when full (Section 8.2.3), an expansion of ~200%, and the urinary bladder distends from ~0.15 liter when empty to ~0.65 liter when full (Table 8.9), a ~333% volume expansion. The spleen may vary in size between 80-300 cm3 largely due to its content of blood, enlarging during digestion (largest in well-fed patients and smallest in starving patients) [5892] – a volume variation of 275%. The uterus of the human female distends massively during pregnancy, enlarging from ~0.1 liter at preconception to >10 liters peripartum (including ~1 liter of uterine wall, ~1 liter of amniotic fluid, and ~3 liters of fetus [4438, 4439]), a ~10,000% expansion of the uterine volume itself though only a 14% addition to total body volume. Note that visceral organs are innervated with spinal visceral afferent neurons that respond to distension, contraction, or other mechanical stimuli [5451] – e.g., excessive bladder distension can induce visceral nociception [5452].) Analyses of nanorobot intrusiveness should add total device volumes to the maximum body system volumes reached in normal functioning if entry and exit take place over one normal functional cycle or longer, with intrusive effect minimized during low-volume phases of the cycle (e.g., during late phases of exhalation and the early phase of inhalation in the lung). The patient’s body volumes may also be actively controlled during nanosurgery (Chapter 12).
Some disease conditions can cause dramatic expansions of organ volumes. For example, in Gaucher’s disease, the liver can enlarge (hepatomegaly) by up to 9 times its normal size (800% volume expansion); liver function is altered, but the impact is usually minor [4440]. The spleen can enlarge up to tenfold during mononucleosis, and Gaucher’s disease also causes an increase in size of the spleen (splenomegaly) up to 20 times its normal size (1900% volume expansion), causing the patient to appear overweight or pregnant [4440]. This splenomegaly is often painless in itself. But the enlarged organ can press on the diaphragm and, indirectly, the lungs, making breathing difficult. It can also press on the stomach and intestines, causing loss of appetite and other digestive problems [4440]. Alcoholic cardiomegaly produces seriously pathological hearts that are enlarged up to 3 times their normal weight (~200% volume expansion) [4441]. Of course, if nanorobot intrusiveness causes significant pathology in a given nanomedical mission design, then that mission design is not viable.
Some body compartments may be less tolerant of volumetric expansion. For example, the typical human eyeball has a volume of ~5.4 cm3 [4442] with an average axial length of 24 mm [4443], but increasing axial length by just 8% to 26 mm may produce myopia, while decreasing axial length by 17% to 20 mm can produce hyperopia [4443]. (There is one extreme report [4444] of an eyeball expanded to a volume of ~31 cm3 due to chronic uveitis and secondary glaucoma in an 18-year-old man.) The peritoneal cavity tolerates moderate stretching. Peritoneal infusion of dialysis patients with 2 liters (3% of body volume) or 3 liters (5% of body volume) of dialysate fluid per washout cycle caused intraperitoneal pressure rises of 13.9 mmHg or 16.8 mmHg in males and 12.1 mmHg or 14.5 mmHg in females, respectively. 64% of patients receiving 2.5 liters and 44% of patients receiving 3 liters reported no physical discomfort, suggesting that somewhat higher volumes could be safely employed [4445].
The interior spaces of joints, bones and the cranial vault in which the brain resides cannot tolerate major intrusions by macroscale foreign objects without surgical assistance. For instance, in joints such as the knee, synovial fluid volume averages 1.1 cm3 (range 0.13-3.5 cm3), so it would seem likely that a maximum ~10% volume displacement of synovial fluid, or ~0.11 cm3 of mechanically-nonirritating foreign objects, would not be intolerably intrusive. One experiment [633] in which canine knee joints received a 0.3% volumetric injection of 3-micron diamond crystals found little evidence of inflammation, with intra-articular pressure and local cell count remaining low. In another experiment [1849], the synovial fluid of rabbit knee joints received an injection of 10- to 20-micron diamond particles in suspension at 5.7% by volume that produced no inflammation. In yet another experiment [902], rats survived implantation of 1- to 8-micron carbon particles in knee even at ~25% of synovial volume. Synovial fluid containing mechanically-irritating needle-shaped monosodium urate (MSU) crystals are diagnostic for gout [4446-4448] at concentrations as low as 0.01-1% by volume.* However, most of the pain and physical disruption of gout arises from the long-term buildup of tophi (large crystalline deposits [4453]) within the affected joint that may ultimately displace 10% or more of the original synovial fluid volume. Knees and other joints are well-supplied with nociceptors [5448], so nanorobots maneuvering in these regions must take care to avoid mechanically inducing sensations of pain.
* This estimate assumes that (a) the crystals measure 0.3-1 micron wide and 15 microns long, (b) there are 10 crystals/leukocyte, and (c) there are 5000-50,000 leukocytes/mm3 of gout-inflamed synovial fluid [4449]. Peritonitis is induced in mice by intraperitoneal injection of ~0.2% by volume of MSU crystals (i.e., 3 mg MSU in a ~1 cm3 cavity [4450]); gouty serum and synovial fluid concentrations of MSU are ~0.01% [4451], while the saturating concentration for phagocytic cells is ~0.03% crystals by volume [4452].
In the brain, normal cerebrospinal fluid (CSF) and intracranial pressure is ~10 mmHg (~0.013 atm), although experimentally-induced excursions up to 100 mmHg (0.13 atm) in primates [4454] or 152 mmHg (0.2 atm) in pigs [4455] have produced neither ischemia nor death. (Intracranial pressure is regulated by the rate of CSF production and resistance to CSF resorption through the arachnoid villi as determined by venous pressure [5489].) The isothermal compressibility of water at 1 atm and 37 oC is kappawater = 4.492 x 10-5 atm-1 [63]. If a brain volume-equivalent of Vbrain = 1400 cm3 of water is placed in a closed incompressible container and pressurized to a maximum safe Pforeign = 0.2 atm by the insertion of an incompressible foreign body of volume Vforeign, then Vforeign ~ kappawater Pforeign Vbrain ~ 0.012 cm3. Substantially larger foreign body volumes may be injected safely into the brain if those injected volumes displace mobile fluids such as cranial CSF. MRI studies [4456] reveal that inhalation of 7% CO2 (producing hypercapnia) induces an average reduction of 9.4 cm3 (range 0.7-23.7 cm3) in human cranial CSF volume, whereas hyperventilation with 60% O2 (producing hypocapnia) induces an average increase in cranial CSF volume of 12.7 cm3 (range 0.7-26.7 cm3). This implies that inert foreign bodies (especially if particulate) up to ~10-20 cm3 in volume (1-2% of brain volume) might safely displace CSF in the brain without ill effect. (Maintenance of blood-brain integrity – a functional intrusiveness issue – is critical.)
Much larger losses of intracranial CSF volume (up to 158.6 cm3 in one patient [4457], or ~10% of brain volume) associated with intracranial hypotension, such as may occur after lumbar puncture procedures or dural tear, can often [4457, 4458] but not always [4459] produce very painful orthostatic headaches (as sometimes occurs in women receiving an epidural anesthetic for childbirth), dural thickening [4460], and other symptoms [4461]. It would be unwise to crowd out the equivalent of the entire cranial CSF volume because the fluid serves an essential function in the brain (Section 8.2.4) – primarily, to cushion the brain in the cranial cavity. M. Sprintz also notes that intracranial pressure is autoregulated within the CNS, so fluctuations in systemic blood pressure will not alter the intracranial pressure within certain blood pressure limits. The prevention of increased intracranial pressure is dependent not only on the autoregulatory system of the CNS but also on the anatomical functionality of the CNS to allow adequate resorption of CSF, thus preventing hydrocephalus and subsequent increased intracranial pressure.
A whole-body tumor load of ~1000-2000 gm (up to ~3% by weight) is generally required for lethality in patients with systemic cancer, whereas in the central nervous system alone a ~100 gm tumor mass (~6% by weight) is lethal [4462]. Depending on their location, solid brain tumors, cerebral mass lesions or intracranial hematomas may produce altered mental function at sizes from a few millimeters [4463] to a few centimeters in diameter [4464], or 0.001-1% of brain volume. In cancer research laboratories, federal (U.S.) regulations require a special permission from OSHA’s affectionately dubbed “mouse police” before a researcher can grow tumors larger than 10% of body weight [4465, 4466] or 1000-2000 mm3 (5-10% of body volume) [4466, 4467], or ascites (serous fluid accumulations in the peritoneal cavity) larger than 20% of body weight [4465], on laboratory test animals. However, tumor lethality is not strictly mass-dependent but is more the result of a loss of organ function and the toxicity of tumor degradation products – benign tumors such as uterine fibroids or myomas can exhibit masses well in excess of the above limits.
Various particle infusions have been tested experimentally. For example, the LD50 for <44-micron alumina particles injected intraperitoneally in mice lies above >2 gm/kg or >0.1% by volume [1067]. All rats survive intraperitoneal injection of 1- to 8-micron carbon particles at 0.1% of body volume [902], and the oral LD50 (the lethal dose needed to kill 50% of the subjects) in rats for PVC powder is >0.7% of body weight [4468] and is 0.8% of body weight for methyl methacrylate powder [4469]. Ceramic powders injected intramuscularly or subcutaneously at >0.5% local tissue volume elicited almost no systemic effects in mice [1067]. A table of standard toxicity classes lists as least toxic or “relatively harmless” to rats a dose of foreign substances having an LD50 of >1.5% of body weight for single oral dose or >2.3% of body weight for skin exposures [4470]. Pathological particulate burdens in lymph nodes may range from 0.07-4% of node volume (Section 15.4.3.4).
In sum, the conservative safe limit for somatic intrusiveness of otherwise biocompatible foreign objects – such as medical nanodevices – is probably in the range of 1-10% of local tissue, organ, or body volume, though larger volumetric expansions may be possible without harm.
From a purely aesthetic perspective, in psychology the limit of human perceptual differential sensitivity for otherwise visually equivalent areas is DeltaAperceptual ~ 0.06 (6%) [4471, 4472]. Thus a human body must change by 6% in visual cross-sectional area to be noticeably different, representing a volumetric change of DeltaVperceptual ~ (1 + DeltaAperceptual )3/2 - 1) ~ 0.09 (9%). For example, the volume added to the human male form by tight-fitting clothing should not create a perceptible increase in body size – wrapping the entire ~2 m2 human skin area with tight-fitting clothing extending ~1.5 mm from the skin surface gives a clothing volume of 0.003 m3 corresponding to a 5% increase in the apparent body volume. Similarly, the volume of a reference male having maximum cyclic lung, stomach and bladder volume exceeds the volume of a reference male having minimum such volumes by ~0.0052 m3, an aesthetically acceptable ~9% volumetric expansion. It is not unusual for body volume to change by ~3%/day due to natural variations in fluid balance and fluid retention. The maximum aesthetic intrusiveness limit thus may be conservatively estimated as 5-10% of basal body volume.
Last updated on 30 April 2004
{kind=link}
{kind=link}