Nanomedicine, Volume IIA: Biocompatibility
© 2003 Robert A. Freitas Jr. All Rights Reserved.
Robert A. Freitas Jr., Nanomedicine, Volume IIA: Biocompatibility, Landes Bioscience, Georgetown, TX, 2003
15.4.2.2 Geometrical Trapping in Liver Vasculature
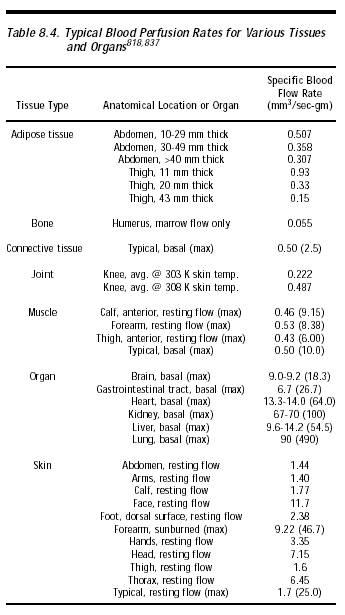
Among the major organs, the liver has the fourth-highest specific blood perfusion rate, typically 10-14 mm3/sec-gm (~1000-1400 cm3/min) up to a maximum of 55 mm3/sec-gm (~5400 cm3/min) (Table 8.4). In the liver, the capillary beds have a high microvasculature number density (Section 8.2.1.2) with the usual vessel diameters. The injection of 15- and 80-micron microspheres directly into the portal vein in rat liver induces embolic portal hypertension, causing venous pressure to elevate 15 mmHg and 24 mmHg, respectively [2690]. One study [2691] found portal vein- and hepatic artery-injected 15-micron microspheres were all trapped in rat liver in both normal and cirrhotic rats. It was claimed that this ruled out intrahepatic shunts larger than 15 microns, but apparently a few ~20-micron intrahepatic shunts from portal vein to hepatic veins, bypassing the sinusoids, are found in cirrhotic human patients [2692]. Another study [2693] found that microspheres at least 40 microns in diameter are required for complete embolization of rat liver.
There are two interesting features of the blood filtration system in the liver that are of potential relevance to medical nanorobot geometrical trapping.
First, the portal venules that supply the liver with blood to be filtered open onto venous sinusoids (Section 8.2.5) measuring 10-13 microns in mean diameter [2725], though varying somewhat with position in the organ [2694, 2697]. This sets a rather large upper limit for clear passage by medical nanorobots. (Mean blood flow velocity through rat sinusoids is 144 (range 54-245) microns/sec, or 197 microns/sec after acute ethanol ingestion [2695], and the varying pressure profile along human liver sinusoids has been modeled [2696].) If sinusoids comprise ~10% of liver volume, then there are ~1000 sinusoids per lobule or ~109 sinusoids in the entire liver, of total tubular length ~1500 km assuming a mean ~100-micron2 cross-section. Sinusoids in periportal areas are narrower, more tortuous, and slightly less porous (5.96% hole area) than the wider, straighter, and more porous (7.94% hole area) centrolobular ones [2697]. Micron-size nanorobots should be able to navigate safely through these passages.
Second, the endothelial cells comprising the sinusoid walls are fenestrated with numerous (5-20 per micron2) small (mean diameter 0.175-micron, range 0.1- to 0.3-micron) openings and fairly rare (<0.1 per micron2) large (0.3- to 1-micron diameter) openings [2697-2700] (Section 8.2.5). These fenestrae are not occluded by diaphragms or basal lamina, hence act as sieve holes through which small nanorobots could possibly be drawn into the 0.5-micron deep Disse space [2701] and thence into the lymphatic drainage. Alternatively, nanorobots could be drawn into direct contact with the microvilli lining the hepatocyte plasma membrane (Section 8.2.5), becoming trapped and possibly endocytosed. Of course, even simple nanorobots equipped with gas concentration sensors (Section 4.2) could probably detect an impending passage into the Disse space because the sinusoid-to-hepatocyte oxygen gradient is 5 mmHg [2702]. Such impending passage may be actively resisted using manipulatory appendages [2762] or by other means (Section 9.4), if required by mission design.
In the narrower periportal sinusoids, red blood cells in transit are forced against the endothelial wall, helping to drive small particles through the holes via “forced sieving” and stirring the fluid in the Disse space via “endothelial massage” [2703, 2704]. The main purpose of the fenestrated endothelium appears to be that of a sieve. The sieve allows the passage of particles <100 nm out of the blood while preventing larger particles, such as ~7-micron-wide red cells and nanorobot-sized ~1-micron chylomicrons, from contacting the hepatocytes [2705-2707]. Chylomicrons are protein-lipid aggregates produced by the intestine and carried by the lymph system into the blood. Their lipids are gradually stripped off by enzymes and their proteins are slowly removed or changed. This causes them to shrink from ~0.5-1 micron in diameter to ~70-80 nm whereupon they can finally pass out of the liver sinusoid through the fenestrae, thence to be absorbed by hepatocytes. The half-life of chylomicrons in the blood is 6-7 minutes [2519-2521], up to 9 minutes in smokers [2520]. The fenestrae thus act to keep the chylomicrons in circulation until they have lost most of their lipid [2707]. Plasma concentration of chylomicrons of various sizes are estimated to range from ~0.5 x 106/mm3 while fasting up to ~50 x 106/mm3 after a large meal, but typically are ~5 x 106/mm3, about the same particle count as red cells. While flowing through blood vessels, chylomicrons are marginated toward the walls [2522] along with the other smallest “flow units” in the blood (Section 9.4.1.3), including nanorobots.
Medical nanorobots larger than 0.3 microns in at least two dimensions are extremely unlikely to be removed from circulation by filtration through the hepatic sinusoidal fenestrae. For smaller nanorobots, it must be noted that the endothelial fenestrae are dynamic cytoskeleton-rich structures [2708] that respond to hormones [2709], viral infection [2710] and cytoskeletal inhibitors [2711-2715], and can be affected by various disease states and local inflammation. It is possible that the size and number of fenestrations [2716-2722] and even the width of sinusoids [2723-2726] could be manipulated via purposeful local biochemical secretions from neighboring medical nanorobots or from other sources.
Last updated on 30 April 2004
{kind=link}