Nanomedicine, Volume IIA: Biocompatibility
© 2003 Robert A. Freitas Jr. All Rights Reserved.
Robert A. Freitas Jr., Nanomedicine, Volume IIA: Biocompatibility, Landes Bioscience, Georgetown, TX, 2003
15.6.2 Bloodstream Intrusiveness
The vascular system is designed to handle large variations in pressure, with the predominant determinant being volume. The issue of bloodstream intrusiveness arises whenever macroscopic quantities of foreign materials or medical nanorobots must be injected into the vascular system, or must be permanently installed or anchored to the wall of a vessel (e.g., Section 15.5.3.6). What is the maximum volume of foreign material that the vascular compartment (e.g., blood, lymph, etc.) can safely accommodate?
The 70 kg reference human male has a red blood cell volume of 36 cm3/kg of lean body mass and ~3.6 cm3/kg of fat [4473]. Assuming the ideal 7% body fat (i.e., typically athletes and models) and a 44% hematocrit (Hct) gives the correct whole blood volume of ~5400 cm3. If the heaviest known human male (485 kg; Section 8.2) had 80% body fat and a 54% Hct, then his whole blood volume may have been ~9.0 liters, or a ~67% (~4 liter) blood volume expansion. The natural limit for arterial wall distension over the physiological blood pressure range from 0.1-0.2 atm is lambdaradial ~ 1.2 radially [4474] and perhaps only lambdalong ~ 1.1 longitudinally, and vein walls are a bit more distensible than arterial walls [3967]. Hence the maximum volume expansion (~length distension x areal distension) of the vascular system at maximum pressure would be at least ~(1 - lambdalong lambdaradial2) = 0.6 (60%). This suggests that a ~4 liter addition to the human blood compartment might be near the maximum limit that natural vascular wall material can accommodate. Again, genetic or other artificial modifications to tissue elasticity or body architecture could further increase the volumetric expansibility of the human vascular compartment.
It is important to note that only a small portion of total body volume is intravascular. A. Meretei speculates that small-gauge intravascular systems can leak access volume to the much larger body volume and thus might become overloaded only very late in the process. Ascites, body-wide edemas and urinary system overload might occur before the vascular systems is stretched to the limits, so the above calculation would be clinically relevant only when we can validly assume no leakage from the intravascular space.
Additionally, minor adjustments occur physiologically:
(1) to red cell volume by the splanchnic tissues [4475] and the spleen (~70 cm3 noncirculating RBC storage volume);
(2) to whole blood volume via shifts between microcirculation and macrocirculation as during hemorrhage compensation (~200 cm3 whole blood [4476]) or dialysis (15.2% whole blood or ~800 cm3 [4477]); and
(3) to blood plasma volume (a) diurnally during sleep (~200 cm3 plasma decrease [4478-4480]), (b) after drinking 1 liter of water (~200 cm3 plasma increase [4480]), (c) during heavy exercise (up to –20% plasma volume decrease or ~600 cm3 [4481-4483]), or (d) after endurance training or heavy exercise (up to +25% plasma volume increase or ~760 cm3 [4484])) such as ultramarathons [4485, 4486].
Patients who lose up to ~2 liters of blood may recover if fluid volume is restored by a transfusion of blood or plasma [4488], or by intravenous infusions of 1.5-2 liters/day of plasma extenders such as 6% hydroxyethyl starch [382]. Recovery is also possible after a loss of up to ~3 liters during gradual exsanguination over a period of 24 hours [4487, 4488]. And plasma volume expansions up to 1.5-3.0 liters are seen in certain pathological conditions such as Waldenstrom’s macroglobulinemia [2484]. However, 1 liter is approximately: (1) the asymptomatic blood loss limit [4488]; (2) the plasma volume change in high-altitude-adapted Andean natives with Hct exceeding 60% [4489]; (3) the hemodilution limit for freshwater aspiration in the lungs [4490]; and (4) the maximum blood collection equivalent (on a relative volume basis) allowed from laboratory animals over a 2-week period (15 cm3/kg or 25% of blood volume [4466]). A volume of 0.5-1.0 liter also is the limit for experimentally-induced [4491] and exercise-induced plasma expansions [4484], hence 10-20% of blood volume appears to be a liberal upper range for nanorobotic volumetric intrusiveness into the bloodstream.
For a more conservative upper range, we note that the acute toxicity of latex microspheres in various nonhuman animals has been investigated experimentally [4492-4498]. For example, all rabbits receiving an intravenous injection of colloidal carbon [2961] or 0.5-micron latex particles [4492] at a blood volume fraction of ~0.1% survived the treatment, and all rats receiving an I.V. injection of 1- to 8-micron carbon particles at a ~0.2% blood volume fraction also survived [902]. As expected, microsphere toxicity due to vascular occlusion is a function of the total volume of microspheres injected [2679] and follows a power law [2679, 4496] of the form NLD50 = Mbody K / Dsphb, where NLD50 is the number of spheres intravenously injected to achieve LD50 in the rat, Mbody is rat body weight in kg, Dsph = microsphere diameter in microns, and the experimentally-determined constants are K = 8.6 x 1011 micron3.15/kg and b = 3.15. Simply extrapolating to a human body weight of Mbody = 70 kg, the LD50 whole-body dose of Dsph = 1 micron latex microspheres would be NLD50 ~ 60 trillion spheres. Consequently taking fblood ~ 0.09 (9%) as the fraction of human body weight represented by blood and rhobody = 1.17 x 10-15 kg/µm3 as the mean human body density, then the human-equivalent LD50 nanocrit (Nct) would be NctLD50 = pi rhobody K / (6 fblood Dsph 0.15) ~ 1%.
However, the above formula for NLD50 is derived mainly from studies of particles >10 microns in diameter (i.e., much larger than medical nanorobots) with varying dimensions and atomically rough surfaces (nanorobots can have identical radii and atomically smooth surfaces), in animal models (rats and beagles) having smaller red blood cell diameters and narrower capillaries than humans. This suggests that humans might be able to tolerate a higher nanocrit of micron-size particles. Additionally, at 0.3% loading with 3-micron microspheres, beagle dogs experienced temporary dyspnea (labored breathing), systemic hypotension and depression of myocardial performance, with the main short-term cause said to be “the large bolus of spheres in the lungs” [2679]. The authors speculated that because smaller spheres are rapidly cleared from the lungs, “reduction of toxicity might be obtained by slow infusion, rather than injection, of these microspheres.” The use of medical nanorobots specifically designed to avoid geometrical trapping in the lungs (Section 15.4.2.1) and the inclusion of respirocyte-class devices [3573] in the injected nanorobot population to forestall ischemic risk (assuming the circulatory pathway is not permanently occluded) should further reduce toxicity.
The human LD50 for microparticles of any kind has not been reported in the literature. The maximum number of PVC contaminant particles allowed in parenteral IV injectable or infusible fluids, according to the British and U.S. Pharmacopoeias, ranges from 1000/cm3 for 2- to 5-micron particles to 5/cm3 for >25-micron particles, or a mere 10-6 - 10-5 % blood volume fraction [4499]. Air-filled bubbles 3-5 microns in diameter stabilized with 25 nm thick half-denatured albumin shells [4500] are diagnostically injected into human patients in the form of a microbubble infusate called Albunex [4501]. Albunex is used as an ultrasound contrast agent [4502] at a concentration of 3-5 x 108 bubbles/cm3 (infusate bubble volume fraction ~ 1%), and infusate doses up to 0.12 cm3/kg of body weight (i.e., 2.5-4.2 x 109 microbubbles injected into the entire human blood volume, producing a whole-body “bubblecrit” equivalent to Nct ~ 0.002%) are said to be well tolerated in man [4503]. Intraarterial administration of very large (40-micron) degradable starch microspheres produces slight early signs of toxicity (nausea/vomiting) in 50% of patients receiving a ~108-particle dose [4504], yielding a blood volume loading equivalent to Nct ~ 0.06% [4504]. The highest reported bacteremic LD50 is ~1010 CFU/ml of blood for an avirulent mutant of S. aureus in mice [4505], an equivalent bacteriocrit to Nct ~ 1% in human blood. Bulk blood viscosity should not be seriously affected by the presence of small microspheres up to Nct ~ 10% (Section 9.4.1.4). We conclude that the safe upper limit of human tolerance for 1- to 3-micron medical nanorobots in the bloodstream probably lies in the range of Nct ~ 0.1-10%. A more exact recommendation must await future laboratory experimental and clinical results.
The intravenous infusion of a maximum 0.540 liter dose (i.e., producing Nct = 10%) of particulate foreign bodies – including all necessary medical nanorobot species required for a particular treatment – suspended in 0.540 liter of aqueous carrier fluid promptly raises blood volume from 5.40 liters to 6.48 liters, elevates blood pressure by ~22 mmHg, and decreases Hct by ~7% (e.g., from 44% to 37%), inducing a temporary mild anemic state unless the foreign particles are oxygen-transporting respirocyte-class [3573] nanorobots (Chapter 22). The addition of >1.0 liter of water to the blood compartment would be required to reduce blood plasma sodium from normal levels at 135-145 mEq/L (3.1-3.3 x 10-3 gm/cm3) to 110-120 mEq/L (2.5-2.8 x 10-3 gm/cm3), sufficient to produce symptomatic hypervolemic hyponatremia and hypokalemia [4506-4508]. Adding just 0.54 liter of excess water should produce only a temporary, nonsymptomatic electrolyte imbalance whose minor effects may be partially offset with ionic amendments to the aqueous carrier fluid. (Utilizing an isotonic aqueous carrier solution should help to avoid causing any electrolyte imbalances.)
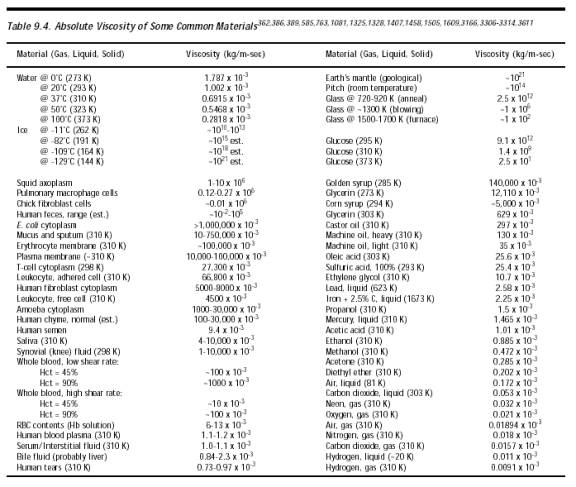
As in cases of mild water intoxication [4509, 4510], following infusion of the maximum 0.540 liter dose the osmoregulatory system should respond by eliminating excess water and electrolytes from the bloodstream via the kidneys and urination. This simultaneously eliminates the modest increase in blood pressure and any electrolyte imbalance while re-establishing normal hematocrit at the cost of slightly elevated blood viscosity (Sections 9.4.1.4 and 9.4.1.5). For non-respirocyte-class nanorobots, the post-infusion equilibrium blood state should approach an Hct of 44%, a maximum nanocrit of 10% (Section 9.4.2.6), a plasma volume reduced from 3.02 liters to 2.48 liters, and a whole blood volume of 5.4 liters. The total particle volume load is then 54%, about equal to the high-end range of Hct for male adults and for newborns [2004]. Nanorobot-infused bulk blood viscosity at 37 oC body temperature rises from ~3.0 x 10-3 kg/m-sec to ~4.8 x 10-3 kg/m-sec in high-shear conditions (Table 9.4, Figure 9.13), which is insignificantly different from 54% Hct whole blood. This increase is not expected to produce whole blood hyperviscosity [4511-4522] as is characteristic: (1) of some anemias [4516], inflammatory diseases [4517], infectious diseases [4511], cerebrovascular diseases [4514, 4519] and certain other conditions [4515, 4520]; or (2) of polycythemia patients who present with hematocrits of 75-85% [4521-4523] which leads to disturbances in blood flow as blood viscosity increases with rising hematocrit. Nor is the viscosity increase likely to induce “blood sludging” [4524] as may occur during shock [4525] or tissue injury [4526, 4527], in which plasma volume is reduced and blood cells tend to agglutinate and form large clumps or masses that move slowly through the vessels, sometimes clogging the smaller vessels [2004]. Osmotic consequences of nanorobot intrusion including ion balance, fluid (and volume) movement, dislocation between body compartments and intracellular, interstitial, and intravascular spaces, and impacts on blood biophysics and chemistry should be systematically addressed, but such a complete analysis is beyond the scope of this text.
Another bloodstream intrusiveness issue is the potential for nanorobot-induced coagulopathy. It is possible that the presence of a sufficiently large concentration of nonadhesive inert microparticles might interfere with the coagulation process by intercalating into the developing thrombus, physically preventing solid clot formation. However, inert polystyrene microspheres are frequently used in coagulation studies [4528] and degradable starch microspheres do not influence platelet aggregation [4529]. The proposed effect has not yet been reported in the literature but could be investigated experimentally.
Last updated on 30 April 2004
{kind=link}
{kind=link}