This document was first published in May 2000 as: Robert A. Freitas Jr., “Respirocytes in Nanomedicine,” Graft: Organ and Cell Transplantation 52(May 2050):148-154 (special “Future Issue,” published May 2000; cover story). It was a contribution to a fictional future issue of the (real world) medical journal Graft in the year 2050. The article was intended to be a fictional retrospective on one aspect of nanomedicine as it might be viewed from a point in time 50 years in the future.
The URL of this document is: http://www.nanomedicine.com/Papers/Graft2050Respirocytes.htm


The Drexler Prize in NanomedicineRespirocytes in Nanomedicine: The Remarkable Story of One of the First Medical Nanorobots Ever ConceivedOn November 6th, 2050, Robert A. Freitas Jr. was awarded the 31st annual Drexler Prize in Nanomedicine during a special interplanetary holo-cast ceremony held in San Francisco, California. The following is a verbatim transcript of the required Prize acceptance speech by Dr. Freitas, as it was delivered in the new Grand Ballroom of the Mark Hopkins Hotel. Mr. Executive Secretary, thank you for that very kind introduction. Ladies, Gentlemen, and Augments, I gratefully and humbly accept the 2050 Drexler Prize in Nanomedicine. As one of the founders of General Nanomedics, I'm directing the Awards Committee to transfer the entire $3 million sum to the Dysneural Society, my favorite charity. They do such excellent work with the only remaining group of patients for whom modern nanorobotic medicine has no good answer—the neurocephalic irreparables. My 98th birthday is exactly one month away, so this is an outstanding birthday gift! [Dr. Freitas holds up a small, transparent crystal statue of a human form.] Of course, there was a time, not so very long ago, that 4 kilos of flawless diamond was worth serious money. Alas, those days are gone! [Audience laughs; Dr. Freitas replaces the statue on the podium.] By now, everyone knows the story of General Nanomedics. How I and a handful of others founded the company in 2006—actually, on the very day Volume III of Nanomedicine came out. How we almost went broke before our first product, DermalZippersNTM, suddenly became a household name. And how our fellow citizens now take utterly for granted all the wonders of modern nanomedicine, everything from instant wound-healing and perfect sex to the utter conquest of classical disease and physiological aging. But few people may recall that my first publication in the field was not the well-known book series, but rather an obscure little paper published two years earlier with the then-preposterous-sounding title "A Mechanical Artificial Red Cell." [A few noises from the audience.] Good, someone actually remembers! That's right, the respirocytes. The paper was published in 1998 by the courageous editor of Artificial Cells [a contemporary medical technology journal] over the anguished howls of protest from several outraged referees.
Not only was this paper the first technical description of respirocytes ever published, it was actually the first technical design description of any medical nanorobot and the very first MedLine entry in nanomedicine! I guess that's one of the reasons I'm here, receiving the award, today. I'm particularly fond of this work because somehow I got almost everything right, at least in the basics, some 13 years before the first commercial prototypes were assembled in our laboratories. As many of you may know, the respirocytes went on to become one of our more important specialty product lines. Even today, decades later, respirocytes continue to be widely used in the fields of emergency and prophylactic medicine, sports and recreation medicine, and of course in space medicine. I'd like to devote the remainder of this talk to reviewing what respirocytes are, and how they came to be, and why I think they are so important.
Molecular NanotechnologyI ask you now to think back to the cold, hard days when nanobiotics and reconfigurable nanoorgans did not yet exist, back to a time before chemoblasts and respirocytes were commonplace—back to the closing years of the 20th century, when nanomedicine was still just a dream in the hearts and minds of a few theoreticians like myself. Generic nanotechnology—that is, progressive miniaturization until you get down to atomic-scale features, commonly known as the "top-down" approach—had first been proposed by Nobel physicist Richard P. Feynman as early as December 1959, in his famous talk entitled "There's Plenty of Room at the Bottom." What is not so often recalled is that in the same talk, Feynman also issued a seemingly "impossible" challenge to build a working electric motor no larger than a 1/64th-inch cube, backed by a $1000 prize out of his own pocket, to spur interest in the project. Just 11 months later, engineer William McLellan had constructed a 250-microgram 2000-rpm motor out of 13 separate parts and collected his reward. Of course, history always repeats. In 1981, K. Eric Drexler first proposed the construction of mechanically deterministic nanorobots starting from atomically-precise molecular parts, the so-called "bottom-up" approach—which came to be known as "molecular nanotechnology." In 1995, Drexler's organization, the Foresight Institute [a charter organization on the Drexler Prize Committee], created a $250,000 Feynman Grand Prize, which was to be awarded to the individual or group that achieved the first design and construction of a working nanometer-scale robotic manipulator arm, along with a functional 8-bit adder computing nanodevice, both of which had to fit entirely inside a 100-nm cube and keep operating for at least 1000 cycles before failing. As you may recall, Dr. James Zyvex demonstrated the first working nanoassembler in 2006 using the "bottom-up" strategy, earning him both the Feynman Grand Prize in 2007 and, a while later, the Nobel Prize in Chemistry, in 2015. But I digress. Even by the mid-1990s, when the respirocytes were first conceived, development successes leading towards true molecular manufacturing and nanorobotics were proceeding along so many independent pathways that it was difficult to keep track of them all. For example, a Scanning Tunneling Microscope was used in 1989 to spell out "IBM" using 35 individual xenon atoms on a nickel surface. By 1995, an Atomic Force Microscope or AFM had performed nanomachining operations on a planar molybdenum trioxide crystals: applying 100 nanonewtons at the tip, two rectangular slots and a 50-nm rectangular sliding member were milled from a crystal, then the member was slid repeatedly from one slot to the other, making a reversible mechanical latch. By 1999, the Molecular Robotics Laboratory at USC was using an AFM to stack up gold nanoparticles like bricks. The chemists were busy too, building a large number of potentially useful rigid nanoparts including molecular-scale rods, rings, springs, cubes, spheres, tetrahedrons, hollow tubes, propellors, and tongs, and wire-frame nanostructures of many shapes made of polymerized DNA. Led by Nobel chemist Jean-Marie Lehn and others, supramolecular chemists began experimenting with molecular "construction kits" and molecular building blocks with fully addressable binding sites that could be used to build up complex three-dimensional well-defined molecular structures. Chemists also manufactured self-assembling multi-nanopart assemblies such as rotaxane "molecular shuttles" which could travel back and forth about 500 times per second in the manner of a molecular abacus; by 1999, the first chemically-assembled electronic nanocomputer logic gates using rotaxanes had been demonstrated by a Hewlett-Packard/UCLA collaboration. Even "top-down" pathways were being avidly pursued. By the mid-1990s, research in Micro Electro-Mechanical Systems or MEMS had produced 100-micron-scale accelerometers, flow valves, pistons, and gear trains, and piezo-driven micromotors were available off-the-shelf in mass quantities. Microgrippers were used to manipulate individual 2.7-micron polystyrene spheres, dried red blood cells, and various protozoa. In 1994, Japanese MEMS engineers at Nippondenso built a 1/1000th-scale working electric automobile just 2.8 millimeters wide—a car the size of a grain of rice—complete with electric motor, wheels, body, spare tire, bumpers, and a 10-micron thick license plate with tiny lettering. This was considered quite a feat, at the time. My own active involvement in medical nanotechnology began in 1994, when I realized that molecular manufacturing promised precise control of matter at the atomic and molecular level. I saw that in just a few decades it would become possible to construct complex machines on the microscopic scale [e.g., 1 micron = 10-6 meter], comprised of parts on the nanometer scale [e.g., about 10-9 meter]. As Drexler had suggested in the 1980s, such tiny machines could be built by assembling in a single device such useful components as 100-nanometer robotic manipulator arms, mechanical GHz-clock computers occupying a cube only 400 nanometers on an edge, molecular sorting rotors for molecule-by-molecule reagent purification spanning a mere 10 nanometers in diameter, and smooth superhard surfaces made of atomically flawless diamond. It seemed obvious that these bacterium-sized nanorobots would profoundly impact the practice of medicine by the early 21st century. For the first time, physicians would be able to perform precise interventions at the cellular and molecular level. The most advanced nanomedical devices would be used to diagnose and eradicate bacterial and viral infections literally in minutes, destroy cancerous tumors with incredible efficiency, eliminate all heart disease, undo metabolic deficiencies, edit or replace the genomes of individual living cells, quickly repair massively traumatized limbs and organs, reverse many forms of neural damage, arrest the aging process, and even restore normal cellular functions after severe freezing injury. However, nanotechnology is such a powerful tool that a little bit goes a long way. Even seemingly modest molecular machine systems may have many applications beyond those which are immediately apparent. To demonstrate this, in 1995 I decided to perform a detailed design analysis of a relatively simple nanomedical device—an artificial mechanical erythrocyte, or "respirocyte"—intended to duplicate all of the important functions of the most common cell in the human body, the red blood cell.
What Red Cells DoFor the benefit of the nonspecialists in the audience I need to say a few words about what red blood cells are, and what they do. Red cells comprise at least 30% of all cells found in the human body. These cells have many useful functions, but they have two most important tasks. First, they must transport respiratory gases throughout the body. Second, they must help prevent the blood from becoming too acidic, since carbon dioxide dissolved in water is an acid. The biochemistry of respiratory gas transport in the blood has been well-understood for more than a century. In brief, oxygen and carbon dioxide [the chief byproduct of the combustion of foodstuffs] are carried between the lungs and the other tissues, mostly within the red blood cells. Hemoglobin, the principal protein in the red blood cell, combines reversibly with oxygen, forming oxyhemoglobin. About 95% of the O2 is carried in this form, the rest being dissolved in the blood. At human body temperature, the hemoglobin in 1 liter of blood holds 200 cubic centimeters of oxygen, 87 times more than plasma alone can carry. Carbon dioxide also combines reversibly with hemoglobin, forming carbamino hemoglobin. About 25% of the CO2 produced during cellular metabolism is carried in this form, with another 65% transported inside the red cells as bicarbonate ion and the remaining 10% dissolved in blood plasma. The creation of carbamino hemoglobin and bicarbonate ion releases hydrogen ions which, without hemoglobin, would leave venous blood 800 times more acidic than arterial blood. This does not happen because hemoglobin reversibly absorbs the excess hydrogen ions, mostly within the red blood cells. Respiratory gases are taken up or released by hemoglobin according to their local partial pressure. There is a reciprocal relation between hemoglobin's affinity for oxygen and carbon dioxide. The relatively high level of O2 in the lungs aids the release of CO2, which is to be expired. The high CO2 level in other tissues aids the release of O2 for use by those tissues.
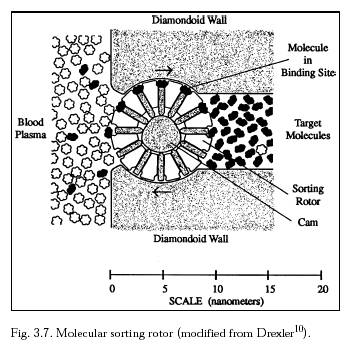
Designing an Artificial Red CellIf we have the ability to precisely engineer complex, micron-scale molecular machine systems, what is the best way to go about designing an artificial red blood cell? Given our goal of oxygen transport from the lungs to other body tissues, the simplest possible design is a microscopic pressure vessel, spherical in shape for maximum compactness. The strongest materials for durable nanostructures include flawless diamond or sapphire, constructed with atomic precision. To a materials engineer, a conservative working stress in such structures would be about 100,000 atmospheres of pressure. But I settled on a standard 1000-atmosphere peak operating pressure for medical devices. This relatively "low" pressure still offers a very high packing density of the gas molecules, while also providing an extremely conservative 100-fold additional structural safety margin. By comparison, natural red blood cells store oxygen at an equivalent 0.51 atmosphere pressure, of which only 0.13 atmosphere is actually deliverable to tissues under normal physiological conditions. How would these microscopic pressure tanks work? In the simplest case, oxygen release could be continuous throughout the body. Slightly more sophisticated would be a system that released gas in response to local O2 partial pressure. But these simple notions fell short on two counts. First, once discharged the devices would become useless. The discharge time is way too short. If there were no natural red cells around to help out, the O2 contained in a 1 cubic centimeter injection of 1000-atmosphere microtanks would be exhausted in only 2 minutes. Second, placement of large numbers of point sources of oxygen emission throughout the capillary bed, side by side with the existing red cell population, causes a serious problem. These extra emitters would be functionally equivalent to red blood cells whose CO2 transport and acid-buffering capabilities had been selectively disabled. Their addition to the blood would push respiratory gas equilibrium toward higher CO2 tension and elevated hydrogen ion concentration. In turn, these higher concentrations would rapidly lead to carbon dioxide toxicity and acidosis [hypercapnia], especially in anemic, nonrespiratory, or ischemic patients, as well as hyperoxic hemolysis and other complications. My solution to the problem of short duration was to continuously recharge the microtanks with oxygen gas at the lungs. I could also prevent carbon dioxide toxicity by providing extra storage for CO2 transport and by designing a mechanism that actively loads the gas in the tissues and then unloads it at the lungs. The key to successful respirocyte function is to provide some active means of conveying gas molecules into, and out of, pressurized microtanks. As early as 1992, Drexler had proposed molecular sorting rotors that would be ideal for this task [Figure 1]. Each rotor has binding site "pockets" along the rim exposed alternately to the blood plasma and the interior chamber by the rotation of the disk. While exposed to blood plasma, a pocket selectively binds a specific molecule like oxygen or carbon dioxide. The disk then rotates so that the loaded binding site moves into the interior chamber. Once the pocket has moved into the chamber, the bound molecule is forcibly ejected by a rod thrust outward by the cam surface. By the 1990s, enzymatic binding sites for oxygen, carbon dioxide, nitrogen, water and glucose were already well known.
More sophisticated molecular sortation systems are available today, but in the late 1990s it was already recognized that Drexler's sorting rotors could be designed from about 100,000 atoms [including the housing], measuring roughly 7 x 14 x 14 nanometers in size. These minute devices could pump small molecules of 20 or fewer atoms at a rate of 1 million molecules/sec against head pressures up to 30,000 atmospheres. Rotors are fully reversible, so they could be used to load or unload gas storage tanks, depending on the direction of rotor rotation. How big should our artificial red cell be? The upper limit is easy to specify because respirocytes must have ready access to all tissues via blood vessels. They cannot be larger than human capillaries which average 8 microns in diameter but may be as small as 4 microns—so narrow that natural red blood cells [7.8 micron x 2.6 micron biconcave disks] must fold in half to pass, single-file. The lower limit, based on minimum component sizes, is about one-quarter micron. I chose a 1-micron diameter for the baseline model. Another design issue was buoyancy, which is easily controlled by loading or unloading water ballast. Why is this important? Active ballast management is crucial when it comes time to remove respirocytes from a patient's blood. Even today, devices are sometimes removed by passing the blood from a catheterized patient into a specialized centrifugation apparatus where acoustic transmitters command respirocytes to establish neutral buoyancy. No other solid blood component can maintain exact neutral buoyancy, as a respirocyte can. As a result, all non-respirocyte blood components precipitate outward during gentle centrifugation and are drawn off and added back to filtered plasma on the other side of the apparatus. Meanwhile, after a period of centrifugation, the plasma, containing mostly suspended respirocytes but few other solids, is drawn off through a 1-micron filter, removing the respirocytes. The reconstituted whole blood returns undamaged to the patient's body. Evidently my paper was the first to propose this process, which today is commonly known as nanapheresis.
RespirocytesThe artificial respirocyte [Figure 2] is a hollow, spherical medical nanorobot exactly 1 micron in diameter. This nanomachine is built of 18 billion precisely arranged structural atoms, and holds an additional 9 billion molecules when it is fully loaded with gas, fuel, and water. Inside, there are two hemispherical storage tanks—one for oxygen and one for carbon dioxide. These surround a third, spherical ballast-water tank of smaller radius that occupies the center of the nanodevice. Each of these three main storage tanks is constructed of diamondoid honeycomb or a geodesic grid skeletal framework for maximum strength. Thick diamond bulkheads separate internal tankage volumes. The outer surface is a biocompatible diamond-sapphire interleaved composite, and a universal "bar code" is embossed around each pole of the device.
Twelve pumping stations are spaced evenly along an equatorial circle. Figure 3 shows the layout more clearly. The large square area in the middle of each station mostly contains molecular sorting rotors for transferring ballast water in and out of the nanorobot. The south and north "wings" of each station are mostly banks of sorting rotors for the loading and unloading of oxygen or carbon dioxide molecules, respectively.
Each station has its own independent 0.3-picowatt powerplant, plus a fuel tank, environmental glucose sensors, and glucose sorting rotors. Power is generated by combining glucose absorbed from the bloodstream with oxygen drawn from internal storage. Any one station acting alone can generate sufficient energy to power the entire respirocyte, and can fully load or discharge any storage tank [whether gas, water, or glucose fuel] in about 10 seconds—a typical capillary transit time in tissues. The power generated onboard mechanically drives the molecular sorting rotors and other subsystems, crudely analogous to various biological motor systems such as the proton pump that drives bacterial flagella or the dynein motor that drives cilia. Each station also has its own set of gas concentration sensors, ambient temperature sensors, and pressure sensors. Figure 4 is one of our earliest SEM images showing a closeup view of an oxygen sensor at top, with the upper half of a temperature sensor also visible at lower left. The attending physician directly controls in vivo nanorobots by broadcasting coded acoustic pulses on ultrasonic frequencies into the body. These high-frequency pulses are received by the pressure sensors and are interpreted as commands or data by the onboard computer. The onboard computer is also necessary for precise control of respiratory gas loading and unloading, rotor field and ballast tank management, glucose engine throttling, power distribution, interpretation of sensor data and commands received from the outside, self-diagnosis and activation of failsafe shutdown protocols, and ongoing revision or correction of protocols in vivo. A 10,000 bit/sec computer with a 1-megabit memory meets all computational requirements, much like the simple chemical process control systems that were used in 20th century factory settings.
Quality control in manufacturing is essential and is strictly monitored by the FDA. Fortunately, nanorobots, like most other digital systems, usually are constructed either structurally correct or seriously flawed. For example, we find that in about one of every trillion respirocyte units the entire rotor subsystem gets omitted, even though all the sensors and bar codes are properly installed, as in Figure 5. These defective devices are very easy for us to detect and remove.
How Do They Work?The average male human body has almost 30 trillion red blood cells, each containing 270 million hemoglobin molecules binding four O2 molecules per hemoglobin. However, since hemoglobin normally operates between 95% saturation (arterial) and 70% saturation (venous), only 25% of stored oxygen is accessible to the tissues. By contrast, each respirocyte stores 1.5 billion oxygen molecules, 100% of which are accessible to the tissues. To fully duplicate human blood active capacity, we must deploy 5.4 trillion devices. If respirocytes are administered via hypodermal injection or transfusion in a 50% aqueous colloidal suspension, this requires a standard 5.6 cubic centimeters therapeutic dose of activated suspension, taking only seconds to inject at, say, an accident scene. One therapeutic dose can duplicate natural red cell function indefinitely if the patient is breathing. It can supply all respiratory gas requirements from onboard storage alone for nearly 2 minutes for patients who are not breathing. One single respirocyte controls nearly the same amount of available oxygen as eight red cells combined, as are shown in Figure 6.
I'm sure any Augment in the audience will agree that one of the greatest benefits of nanomedical devices is their ability to extend natural human capabilities. Suppose you want to permanently maximize the oxygen-carrying capacity of your blood by infusing the largest possible number of respirocytes. The maximum safe augmentation dosage is about 1 liter of 50% respirocyte suspension, producing a 9% respirocrit. This puts nearly a quadrillion devices into your bloodstream, allowing you to hold your breath for almost 4 hours at the normal resting metabolic rate. At the maximum human metabolic rate, which is something like a continuous Olympic-class 50-meter dash exertion level, you could go for a full 12 minutes without taking a breath if you can also uptake the excess lactate and deal with a few other minor problems. Afterwards, your entire oxygen transport capacity is recharged by hyperventilating for just 8 minutes—and then you're ready to go again! All this is familiar to sports buffs, who will undoubtedly recall that it was evidence of widespread respirocyte blood doping during the notorious XXIX Summer Olympics in 2016 which ultimately resulted in the emergence of the first separate "Auggie Olympics" during the regular XXX Olympiad in 2020.
Are They Safe?The original design study noted that respirocyte self-diagnostic routines would detect simple failure modes like jammed rotor banks or gas leaks, either switching to backup systems or using those backups to safely place the device into a fail-safe dormant mode pending removal by nanapheresis. But respirocytes were expected to be extremely reliable. A simple analysis of likely radiation damage suggested that the average respirocyte should last about 20 years before failing due to radiation-induced defects. But what if all 12 glucose engines jammed on and refused to turn off? If this malfunction occurs while the respirocyte is in your bloodstream, device temperature won't rise at all. That's because the 7.3 picowatts of continuous thermal energy the device is generating is easily absorbed by the huge aqueous heat sink, which has a bountiful heat capacity. During lectures in the old days, someone would always ask me from the back row: Can respirocytes explode? And I would tell them that each device contains up to a quarter cubic micron of oxygen and carbon dioxide gas at 1000 atmospheres of pressure, representing 24 picojoules of stored mechanical energy. If the device explodes in air the shrapnel travels outward at ~257 meters/sec, slower than the speed of sound in air [331 meters/sec] so there is no acoustic shock wave—it will hiss, not snap. If the device explodes inside human tissue, the gases do work against the surrounding fluid, displacing 100 cubic microns of water while raising local temperature only 0.04oC and expanding a gas bubble less than 6 microns in diameter, just 2% the volume of a typical human tissue cell. Since the average separation of neighboring respirocytes in the blood is 2-10 microns [depending on dosage], such gas bubbles should be reabsorbed almost immediately. So single-device explosions are unlikely to cause embolic or other significant damage. This expectation was borne out during our Phase I trials, and subsequently by more than three decades of clinical experience with the device. Short of manufacturing defect, it's pretty hard to imagine a scenario that leads to complete structural failure of a respirocyte in vivo. Patients suffering a multistory fall onto a concrete pavement or a high-speed head-on automobile collision experience instantaneous accelerations of 100-10,000 g's [gravity is 1 g], but a spherical diamondoid shell resists accelerations up to 0.1-10 billion g's. Crushing respirocyte-impregnated human tissue in an hydraulic press is unlikely to destroy any devices, as they will simply slide out of the way. The same logic applies to gunshot wounds, knife accidents that cut deep to hard bone, and blunt object blows to the skull. Indeed, the only plausible respirocyte explosion scenario I could come up with was dental grinding. That's because tooth enamel is the hardest natural substance in the human body, and a patient with an oral lesion can spread respirocyte-impregnated blood over the teeth. Single-device explosions just aren't detectable. In the original paper, back in 1998, I estimated that several thousand orally-crushed respirocytes going off all at once might produce a "fizziness" in the mouth. Simultaneously crushing 20 million respirocytes [the total count in a 0.5-mm droplet of augmentation-dose blood] could in theory produce a maximum jaw-speed[0.1 m/sec] explosive impulse. Of course, this requires 100% crushing efficiency, and the out-of-bloodstream protocols all have to fail simultaneously in all devices, an astronomically rare event. Actually, I did see a case like this reported once in the literature, back in the early 2030s. Was it the Journal of Oral and Maxillofacial Surgery where I saw it? Some kind of strange frat house initiation ritual, as I recall, with all of the respirocyte safety protocols autogenously disabled by the victims. Of course, alcohol was involved.
Applications AplentyThe mechanical respirocyte was first used as the active oxygen-carrying component of a universally transfusable and completely recyclable blood substitute certifiably free of disease vectors such as hepatitis, venereal diseases, malarial parasites and HIV. It could be stored indefinitely and was readily available to recipients of all blood types. Organ donation also got a boost. In the early decades of this century, organs still had to be transplanted reasonably soon after harvest. Respirocytes could be employed as a long-duration perfusant to help preserve living tissue, especially at low temperature, for grafts [kidney, marrow, liver and skin] and for organ transplantation. But with the development of cell mills in the 2020s and organ mills in the 2030s, isogenetic human cells and organs could be quickly manufactured to personal specifications in clinical settings and so this application for respirocytes has declined. Respirocytes also were initially used as a complete or partial symptomatic treatment for virtually all forms of anemia. The devices were a good preventative treatment for perinatal and neonatal disorders such as Sudden Infant Death Syndrome [SIDS] or crib death, the leading cause of neonatal death in the U.S. at the close of the 20th century. Respirocytes also helped in the treatment of a wide variety of lung diseases and conditions ranging in severity from hay fever, asthma and snoring to tetanus, pneumonia and polio. But today we have complete cures for all of these classical diseases, so respirocytes are now used in these cases only for temporary symptomatic relief. Respirocytes also contributed to the success of certain extremely aggressive cardiovascular and neurovascular procedures, tumor therapies, and diagnostics that were popular in the early decades of this century, though with the development of vasculomobile repair nanorobots such as the endotheliocytes this application has also declined in importance. Of course, respirocytes make it possible to breathe in oxygen-poor environments, or in situations where normal breathing is obstructed or physically impossible. This remains the most popular application for respirocytes today. Prompt insertion of a therapeutic dose by emergency personnel, or advance infusion with an augmentation dose, greatly reduces the number of choking injuries and deaths, and has almost eliminated the use of such barbaric 20th century techniques such as tracheostomies, tracheal intubation and mechanical ventilators, and "artificial respiration" during first aid. Respirocytes provide an excellent prophylactic treatment for most forms of asphyxia, especially those involving drowning, strangling, electric shock [some respirocytes are purely mechanical], nerve-blocking paralytic agents, carbon monoxide poisoning, underwater rescue operations, smoke inhalation or firefighting activities, anaesthetic or barbiturate overdose, confinement in airtight spaces [traditionally refrigerators, closets, bank vaults, mines, and submarines], or mechanical obstruction of breathing [by a chunk of meat or a plug of chewing tobacco lodged in the larynx, by inhalation of vomitus, or by a plastic bag accidentally pulled over the head of a child]. An interesting alternative to augmentation infusions is a therapeutic population of respirocytes that loads and unloads gases at an artificial nanolung, a large diamondoid pressure tank implanted in the chest. The chest tank exchanges gases directly with the natural lungs or with an external gas supply such as an air hose. With about 80% storage volume at ~1000 atmospheres, an unobtrusive 250 cubic centimeter petite nanolung provides 0.3 to 7 hours of O2 supply, depending on exertion level. By sacrificing one entire natural lung to make room in the thorax, a 3250 cubic centimeter full nanolung extends oxygen supply to 4-87 hours. This application is very popular in our orbital cities, because it allows people to live and work in space wearing nothing but thin-walled compression skinsuits. I hear that less-conservative military nanolungs allow emergency survival for up to 5 days without drawing a breath. Do we have any Augments with commercial nanolungs in the audience? Show of hands—one, two,...three? That's pretty typical. As I've already mentioned, respirocytes allow dedicated athletes to achieve major new sports records. That's because the devices can deliver oxygen to muscle tissue far faster than maximum lung capacity, essentially for the duration of the sports event. The original baseline respirocyte design promised to deliver over 200 times more oxygen to the tissues per unit volume than natural red cells, and also promised a similar advantage in carbon dioxide transport. Our latest model, the Mark VIII, does about three times better than this. The respirocyte has had a huge impact in running, swimming, and other endurance-oriented events, and in competitive sports such as basketball and soccer where extended periods of sustained maximum exertion are required. I believe the 2-minute mile was just broken last year by a trans-female Augment from Kenya—I'm sorry but I can't recall her name right now. The respirocytes have also found wide use in veterinary medicine, especially in cases of vehicular trauma and kidney failure where transfusions were traditionally required; and also in battlefield applications demanding rapid blood replacement or personnel performance enhancement, though fortunately battlefields are getting pretty rare these days. Swallowed in pill form, our GasNixNTM respirocyte-derived product is an effective, though temporary, cure for flatulence, acid reflux and eructation. Another early spinoff of respirocyte technology was the pharmacyte, an ingestible or inhalable medical nanorobot that provides precisely timed and scheduled systemic biochemical releases. There is much more I could say, but I see that the Executive Secretary is waving frantically and gesturing at his wristwatch, so I suppose my time here is already done. [Audience titters.] So I'll just wrap this up by thanking you all for coming here and sharing this sunny winter day with me. This is really a wonderful old hotel. My wife and I spent our first night of married life in this hotel, in a cozy little room with an unforgettable view about 10 stories up from where I'm standing here—and we just celebrated our 75th anniversary last year. Does anyone recall what you're supposed to give your wife on your 100th anniversary? No? Well, whatever it is, I'm sure she'll let me know. [Audience laughs.] Thank you again, Ladies, Gentlemen, and Augments, and also my most sincere thanks to the Awards Committee for honoring me as the winner of the 2050 Drexler Prize in Nanomedicine. [Audience stands and applauds.]
CosmoNet Press Package, Additional Background Information: Dr. Freitas' original research paper on respirocytes was first published in the 20th century technical academic print media, on 15 July 1998, as: Robert A. Freitas Jr., "Exploratory Design in Medical Nanotechnology: A Mechanical Artificial Red Cell," Artificial Cells, Blood Substitutes, and Immobil. Biotech. Vol. 26, No. 4, 1998, pp. 411-430. A more complete version of this classic early work may still be viewed in the ancient Internet Archives, indexed under the old-format "Uniform Resource Locator" or "URL" at: http://www.foresight.org/Nanomedicine/Respirocytes.html.
|
Last updated 24 July 2004