Nanomedicine, Volume IIA: Biocompatibility
© 2003 Robert A. Freitas Jr. All Rights Reserved.
Robert A. Freitas Jr., Nanomedicine, Volume IIA: Biocompatibility, Landes Bioscience, Georgetown, TX, 2003
15.4.3.6 Phagocyte Avoidance and Escape
Invading microbes that readily attract phagocytes and are easily ingested and killed are generally unsuccessful as parasites. In contrast, most bacteria that are successful as parasites interfere to some extent with the activities of phagocytes or find some way to avoid their attention [3302]. Bacterial pathogens have devised numerous diverse strategies to avoid phagocytic engulfment and killing. These strategies are mostly aimed at blocking one or more of the steps in phagocytosis, thereby halting the process [3302].
Similarly, phagocytic cells presented with any significant concentration of medical nanorobots may attempt to internalize these nanorobots. How often will such an opportunity arise? There are an average of one ~730-micron3 granulocyte or PMN in every ~3 x 105 micron3 of human blood, one ~1525-micron3 monocyte in every ~2 x 106 micron3 of blood, and one >1525-micron3 macrophage in every ~2 x 105 micron3 of human tissues. By random thermal motions in a quiet fluid, a 2-micron nanorobot would trace out a volume containing one PMN in ~70 sec at 37 oC (Eqn. 3.1), or would diffuse the ~40-micron mean free distance (Eqn. 9.72) between nanorobot and the nearest macrophage in quiet watery tissue in ~4000 sec (Eqn. 3.1). In a small (1 mm diameter) artery with blood flowing at 100 mm/sec, each 2-micron nanorobot, in a total bloodstream population of 1012 such nanorobots, would collide with a PMN cell once every ~3 seconds near the periphery of the vessel but only once every ~300 seconds near the center of the vessel (Section 9.4.2.2). This rheological disparity will be amplified by phagocyte margination (Section 9.4.1.3) and nanorobotic vascular plasmatic zone locomotion (Section 9.4.2.6). Studies of macrophage particle-ingestion kinetics show that the number of particles ingested by each phagocytic cell may rise tenfold as the local particle concentration rises from 5 particles per cell to 150 particles per cell [1074].
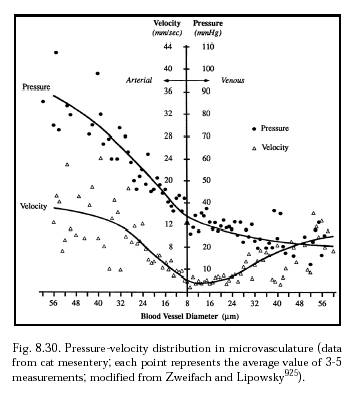
From these crude estimates – which neglect the effects of variable blood flow rates (Figure 8.30), large-vessel turbulence (Section 9.2.5), and other factors – it becomes apparent that virtually every medical nanorobot placed inside the human body will physically encounter phagocytic cells many times during its mission. Thus all nanorobots that are of a size capable of ingestion by phagocytic cells must incorporate physical mechanisms and operational protocols for avoiding and escaping from phagocytes [26, 27]. Engulfment may require from many seconds to many minutes to go to completion (Section 15.4.3.1), depending upon the size of the particle to be internalized, so medical nanorobots should have plenty of time to detect, and to actively prevent, this process.*
* Detection by a medical nanorobot that it is being engulfed by a phagocyte may be accomplished using (1) hull-mounted chemotactic sensor pads equipped with artificial binding sites that are specific to phagocyte coat molecules, (2) continuous monitoring of the flow rates of nanorobot nutrient ingestion or waste ejection mechanisms (e.g., blocked glucose or O2 import), (3) acoustic techniques (e.g., Section 4.8.2), (4) direct measurement of mechanical forces on the hull, or (5) various other means.
The basic strategy is first to avoid phagocytic contact (Section 15.4.3.6.1), recognition (Section 15.4.3.6.2), or binding and activation (Section 15.4.3.6.3), and secondly, if this fails, then to inhibit phagocytic engulfment (Section 15.4.3.6.4) or enclosure and scission (Section 15.4.3.6.5) of the phagosome. If trapped, the medical nanorobot can induce exocytosis of the phagosomal vacuole in which it is lodged (Section 15.4.3.6.6) or inhibit both phagolysosomal fusion (Section 15.4.3.6.7) and phagosome metabolism (Section 15.4.3.6.8). In rare circumstances, it may be necessary to kill the phagocyte (Section 15.4.3.6.9) or to blockade the entire phagocytic system (Section 15.4.3.6.10).
Of course, the most direct approach for a fully-functional medical nanorobot is to employ its motility mechanisms to locomote out of, or away from, the phagocytic cell that is attempting to engulf it. This may involve reverse cytopenetration (Section 9.4.5), which must be done cautiously (e.g., the rapid exit of nonenveloped viruses from cells can be cytotoxic [5356]).
It is possible that frustrated phagocytosis may induce a localized compensatory granulomatous reaction. Medical nanorobots therefore may also need to employ simple but active defensive strategies to forestall granuloma formation (Section 15.4.3.5).
Last updated on 30 April 2004
{kind=link}